Virtual Assistant Lab Orders and Scheduling: What Your Clinic Can Delegate
Virtual assistant lab orders and scheduling support addresses two of the most visible failure points in daily clinic operations. When lab follow-up slips, care is affected. When scheduling is inconsistent, the day starts behind and stays there. These are not occasional problems. They are the predictable result of asking staff to manage high-volume, time-sensitive administrative functions as a side task alongside everything else they are responsible for.
The short answer to whether a VA can handle both is yes. The more useful answer is what that looks like in practice, where the clinical line sits, and how the arrangement actually fits into the systems a clinic already runs. A medical virtual assistant in either role takes over the administrative layer and keeps it moving. Here is exactly what falls within scope.
TL;DR: Can a Medical Virtual Assistant Manage Lab Orders and Patient Scheduling?
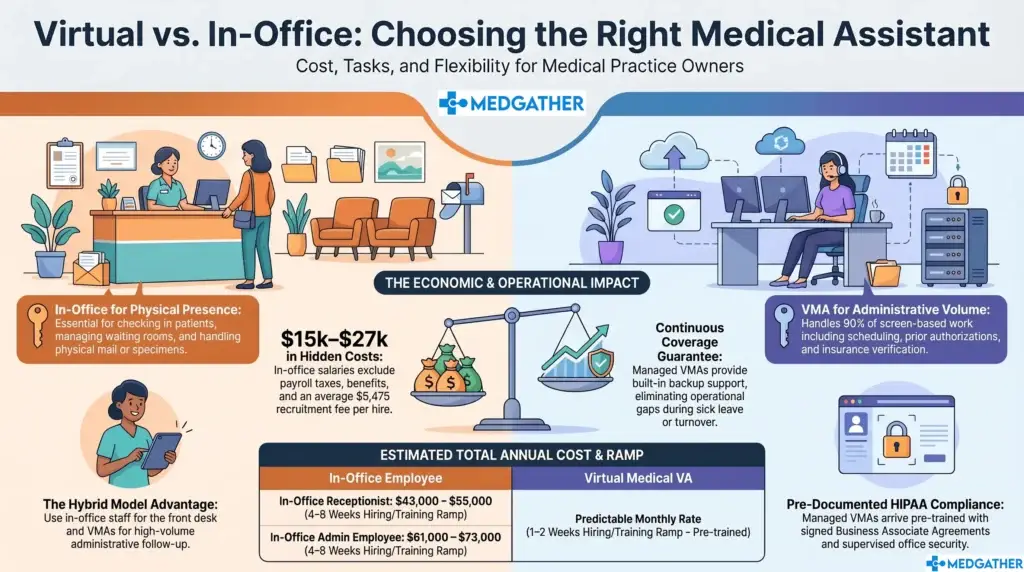
Yes. A medical virtual assistant (VA) can manage the administrative side of lab order coordination and patient scheduling, helping practices keep workflows organized and reduce delays. Responsibilities include scheduling appointments, confirming visits, managing waitlists, tracking lab orders, following up on pending results, and ensuring documentation is complete before providers take clinical action.
Medical virtual assistants do not interpret test results, diagnose conditions, prescribe treatment, or communicate clinical findings to patients. Those responsibilities remain with licensed healthcare providers. By handling routine administrative work, VAs help reduce no-shows, improve workflow efficiency, and allow front desk staff to focus on patients in the clinic.
MedGather’s office-based medical virtual assistants work from secure, managed facilities using company-issued devices and HIPAA-compliant processes, providing healthcare practices with reliable administrative support while helping safeguard patient information.

Board-certified gastroenterologist and Founder of MedGather. Read full bio →
What This Support Covers
Lab Order Coordination
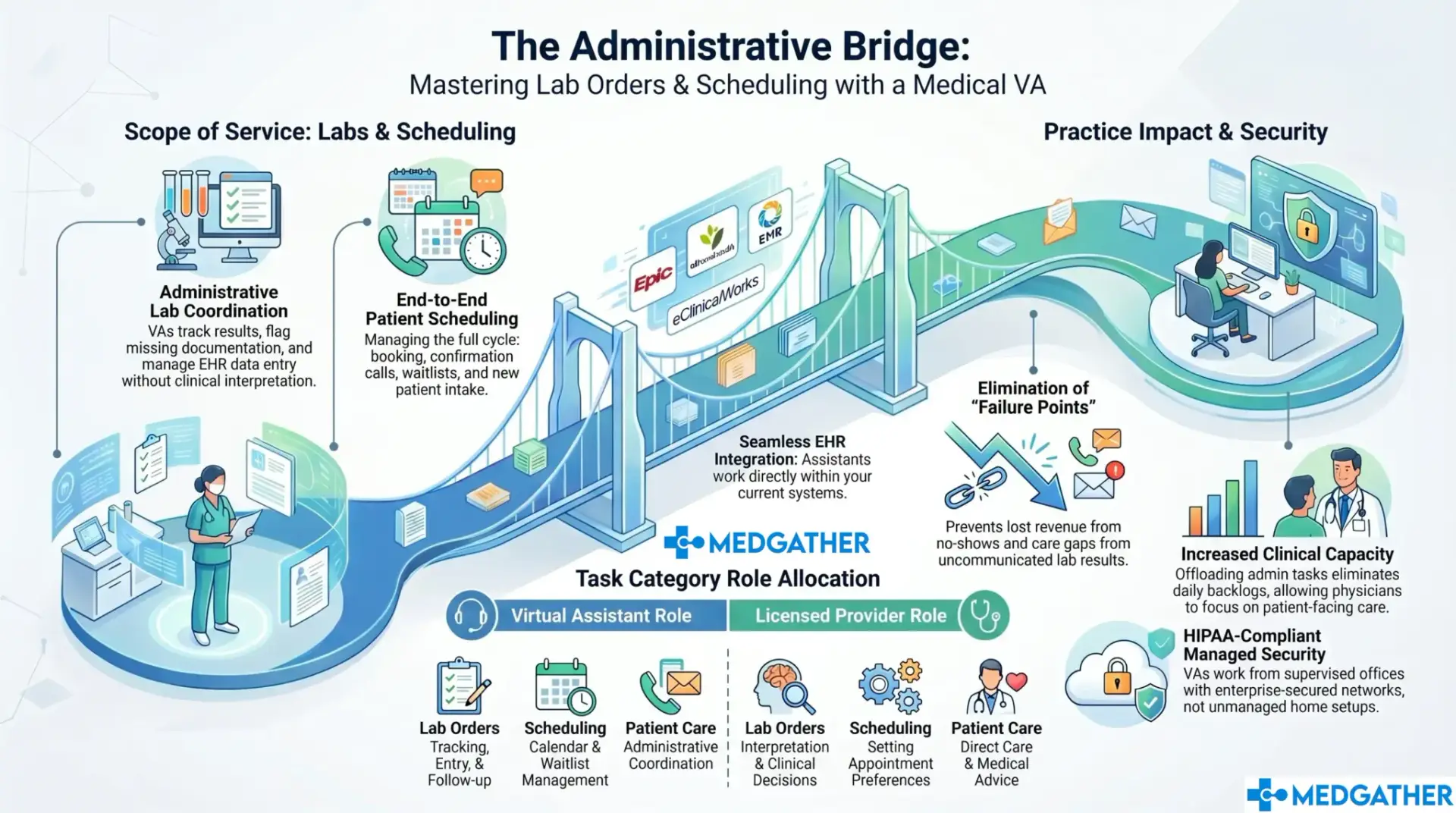
Lab support at the administrative level means coordination and tracking. Not clinical decisions. The VA follows up on pending results, makes sure orders are entered accurately in the EHR, flags incomplete or missing documentation, keeps the relevant staff updated on status, and manages communication between the clinical team and the laboratory when responses are delayed or results are unclear.
The clinical judgment stays entirely with the physician. The VA does not interpret results, make clinical recommendations, or communicate lab findings to patients without explicit direction. What they do is make sure nothing falls through on the administrative side: that the order was placed, that the result came back, that it was entered correctly, and that the right person was notified.
This distinction matters when practices are evaluating scope. A full breakdown of which tasks fall within remote support and which stay in-house follows a consistent pattern across most clinic types. The administrative layer around any clinical function is where a trained VA adds value. The clinical decision itself always stays with the licensed provider.
For practices running high lab volumes, such as endocrinology, oncology, or internal medicine, dedicated lab coordination removes a recurring drain on clinical staff time. When a nurse is no longer spending part of every afternoon chasing lab results, their capacity for patient-facing work increases directly. The math is straightforward. The impact is felt the first week.
Patient Scheduling
Scheduling covers more ground than most clinics fully account for when it is managed manually. Appointment booking, rescheduling, confirmation follow-ups, waitlist management, new patient intake, and provider-specific scheduling preferences all require consistent, attentive management throughout the day.
The complexity of scheduling grows with practice size. A clinic managing multiple providers, each with different availability windows, referral preferences, and appointment types, is running a scheduling operation that benefits from someone whose entire job is exactly that. When scheduling is managed by whoever has a free moment, errors accumulate and the calendar becomes reactive rather than managed.
Both lab coordination and scheduling require EHR familiarity. MedGather’s VAs are trained across Epic, Athenahealth, eClinicalWorks, and Modmed, and complete client-specific workflow training before handling any tasks. The practice does not need to change its systems or workflows to accommodate remote support.
Why These Two Functions Matter So Much
Lab follow-up gaps affect patient care in ways that are often not visible until the damage is done. A result that was not communicated, an order that was placed but never tracked, a patient who called for an update and reached voicemail. These are not isolated incidents. They are the predictable outcome of an administrative function with no clear owner.
Scheduling handled inconsistently means unfilled slots, double-bookings, and no-shows that would have been prevented with a confirmation call. The calendar starts each day already behind. The practice absorbs the cost without always connecting it back to the scheduling function that caused it.
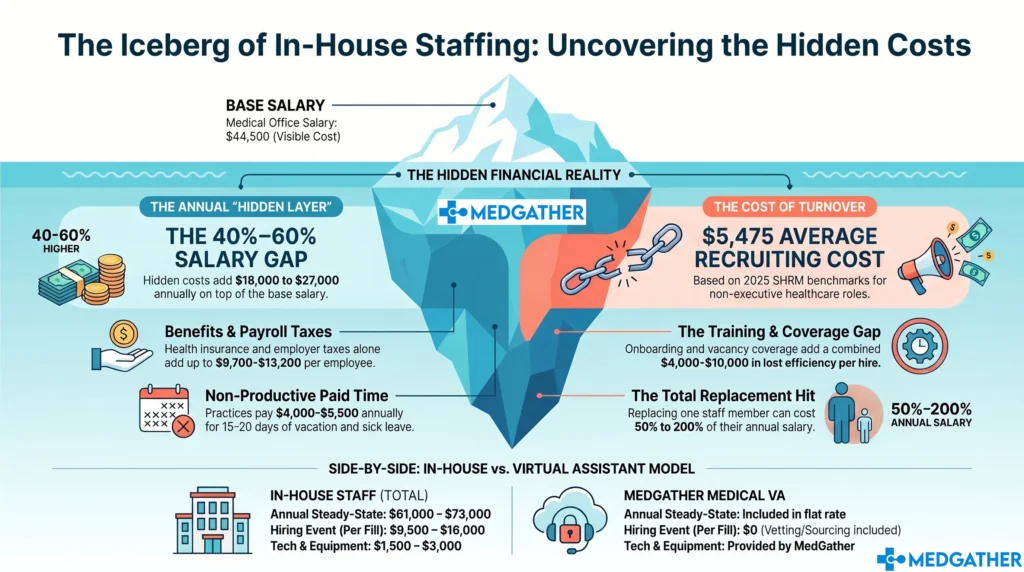
Delegating these functions to a trained assistant keeps them structured without adding to on-site headcount. For practices already stretched at the front desk, it means fewer things fall through during busy periods. How in-house staffing costs compare to virtual support once the full picture is calculated makes the financial case clearer than a surface-level rate comparison. The real question is not what the hourly rate is. It is what the gap costs when nobody owns the function consistently.
There is a patient experience dimension to this that does not always get factored into the operational calculation. Patients who receive consistent confirmation outreach show up at higher rates. Patients whose lab results are communicated promptly and accurately trust the practice more. The administrative function, when it runs well, is invisible. When it does not, patients notice it before anything else.
Benefits for Your Practice
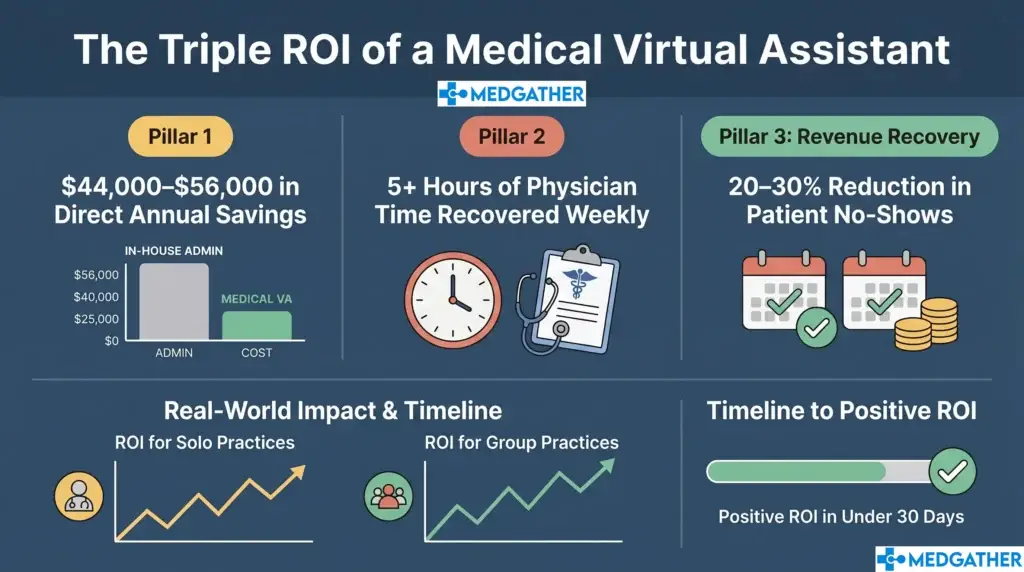
Physicians and clinical staff spend a significant portion of each day on work that does not require their clinical expertise. Offloading lab coordination and scheduling to a trained assistant creates room for patient care. For a physician seeing patients back to back, that room is not abstract. It is the difference between finishing the day caught up and finishing with an hour of administrative backlog still ahead.
For front-desk teams at capacity, a VA handling scheduling removes the constant context-switching that causes delays during peak periods. When the scheduler is someone whose primary responsibility is scheduling, the calendar gets managed rather than managed around everything else. Confirmation calls go out. Waitlist slots get filled. New patient intake arrives before the appointment instead of during it.
Consistent scheduling support also compounds. As the assistant learns the practice’s patient population, provider preferences, and peak volume patterns, the scheduling function improves over time rather than staying flat. How this fits into a broader strategy for reducing administrative workload gives the fuller operational picture before any remote support arrangement is set up.
Lab coordination has a similar compounding effect. An assistant who has been managing a practice’s lab tracking for six months knows which payers are slow, which tests generate frequent follow-up calls, and which providers want status updates in what format. That context is not something that gets rebuilt quickly when it walks out the door.
Common Concerns
Accuracy is the primary concern around lab tracking, and it should be. Errors in this function carry real clinical consequences. MedGather addresses this through a low-error standard applied across all administrative work, a supervised team model where oversight is built into the daily workflow, and client-specific training before any assistant handles patient information or lab coordination. The standard is not self-reported. It is enforced structurally.
HIPAA compliance is the other concern that comes up consistently. Remote access to scheduling systems and EHRs means the environment the assistant works in matters as much as their individual training. An assistant on a personal device on a home network, without managed access controls or device management, is a compliance liability regardless of how capable they are.
MedGather operates from a managed, supervised office environment with stable infrastructure, enterprise-secured networks, and backup systems in place. How MedGather’s office-based model keeps remote access secure covers what that environment looks like in practice and why the operating model matters as much as the individual’s qualifications.
A third concern that comes up in practices with complex provider configurations is whether one assistant can manage the scheduling preferences of multiple providers simultaneously. The answer depends on volume and workflow complexity. MedGather’s onboarding briefing covers provider-specific preferences, scheduling protocols, and escalation rules before any assistant takes on independent scheduling tasks.
How MedGather Approaches This
MedGather’s VAs integrate into the scheduling and lab tracking processes the clinic already has rather than introducing parallel systems or requiring workflow changes. For scheduling, that means fitting into the existing booking setup, following the practice’s confirmation protocols, and managing the calendar within the systems already in use. For lab coordination, it means operating through the EHR structure the clinic already relies on.
The goal is to take over the administrative function without creating a transition period where things fall further behind. The onboarding process is designed to front-load the practice-specific briefing so the assistant is managing the function effectively from the first week, not building toward effectiveness over months.
What remote support looks like across a full range of administrative functions, including how each specific task is handled within a supervised model, gives the broader picture of where lab coordination and scheduling sit within a full engagement.
For practices that have tried freelance or unstructured arrangements before and found the consistency lacking, the distinction with MedGather is structural. The oversight is built into how the team operates every day, not left to the individual assistant’s self-management. When a step gets missed, there is a supervision layer to catch it. When a workflow needs to change, the documentation lives in the team, not with one person who might not be there next month.
Running a clinic is already a full-time job.
You should not have to carry the administrative side of it alone. Book a free strategy call and we will help you figure out exactly where remote support fits your workflow.
Frequently Asked Questions
Does a virtual medical assistant handle the actual lab orders or just the coordination?
The role covers the administrative side: tracking, data entry, flagging incomplete documentation, and follow-up. Clinical decisions around ordering and interpreting results stay with the physician. Which tasks fall within remote support and which stay in-house follows a consistent pattern across most practice types. The line between administrative coordination and clinical decision-making is clear and consistently maintained.
Can one assistant manage scheduling for a multi-provider clinic?
It depends on volume and how scheduling is currently set up. VAs are trained to handle high-volume tasks and briefed on provider-specific preferences during onboarding. What the hiring and onboarding process looks like is worth reviewing early so expectations on both sides are clear before the assistant starts. Some multi-provider practices find one assistant covers everything effectively. Others with very high volume benefit from discussing a more structured scope.
How does a remote assistant access our scheduling system securely?
Access runs through the clinic’s existing EHR or scheduling platform. MedGather operates from a HIPAA-compliant, supervised office environment with stable infrastructure and backup systems in place. How compliance is maintained across remote healthcare support covers the security structure in practice. The clinic retains full control over access permissions, and access is granted and documented according to the clinic’s own protocols.
Is this different from hiring an in-house scheduler?
The day-to-day tasks overlap, but the structure is different. A remote VA is part of a supervised team, which changes how consistency and accountability are maintained over time. An in-house hire who leaves takes the institutional knowledge of the scheduling function with them. The MedGather model documents workflows at the team level, so transitions do not reset what the practice has built. What that difference looks like operationally is worth reading before making a staffing decision.