Medical Virtual Assistant for Busy Clinics: 5 Ways to Stop the Administrative Spiral
There’s a version of a busy clinic that looks fine from the outside. Patients are coming in, appointments are being booked, and the team is showing up every day.
But underneath that, someone is staying late to finish documentation. Someone else is covering two roles because the last hire didn’t work out. And the front desk is managing a call queue, a scheduling backlog, and a stack of prior authorization follow-ups all at the same time.
That’s not a staffing problem. That’s a structural one.
A medical virtual assistant for busy clinics is built to address exactly that structure. Not by replacing your team, but by absorbing the administrative layer that’s pulling them in too many directions at once. The role a medical virtual assistant plays in a modern practice is broader than most clinics realize when they first start looking at the model.
In This Guide
- Why busy clinics have a structural problem, not a staffing one
- The numbers behind the burnout
- What happens when you stop relying on retraining
- 5 areas where a medical virtual assistant makes the biggest difference in a busy clinic
- What to expect when you bring one in
Why a Medical Virtual Assistant for Busy Clinics Addresses a Structural Problem
Dr. Ruel Garcia founded MedGather because that reality was playing out in clinics across the country. The administrative workload was landing on the wrong people, pulling clinical staff away from patients, and quietly burning teams out. The answer wasn’t more pressure on existing staff. It was structured, reliable support that could absorb the administrative layer without disrupting how the clinic already operated.
That distinction matters. A lot of busy clinics respond to administrative overload by redistributing the work across existing staff, extending hours, or cycling through new hires who burn out just as fast as the ones they replaced. The problem is that none of those responses change the structure. They just move the pressure around.
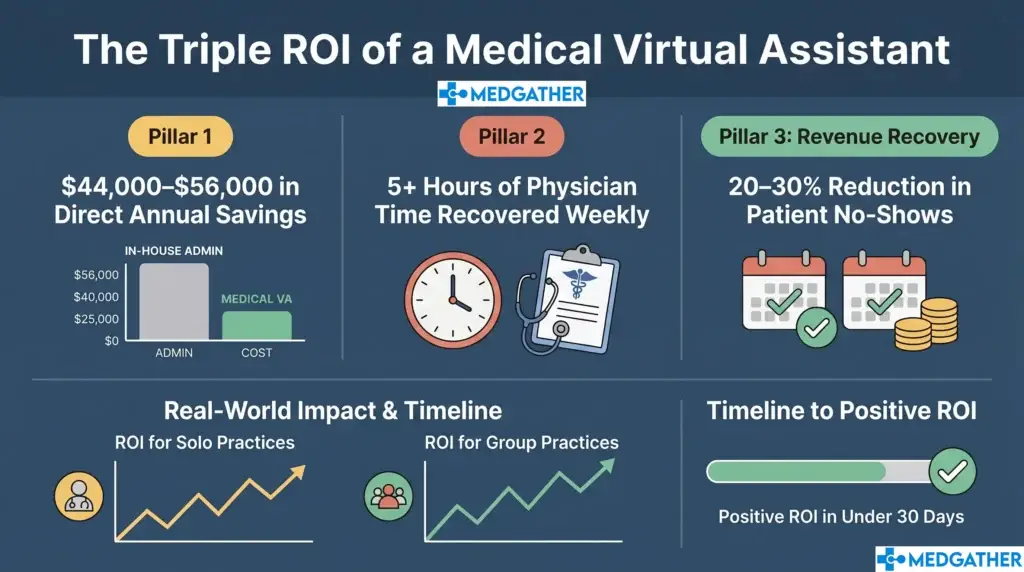
A medical virtual assistant changes the structure. The administrative layer gets a dedicated owner. The clinical team gets to focus on clinical work. And the practice stops losing capacity every time someone decides the workload isn’t worth staying for. How that shift affects practice efficiency on a measurable level is something most practices only see clearly after they’ve experienced it for 60 to 90 days.
The Numbers Behind the Burnout
The data on healthcare staff burnout is not subtle, and it is not improving.
A 2022 report from the American Nurses Association found that nearly half of nurses surveyed reported feeling burned out, with administrative burden cited as a primary contributor alongside direct patient care demands. The workload was not just heavy. It was the wrong kind of heavy: the kind that doesn’t directly connect to why most clinical staff went into healthcare in the first place.
The Advisory Board’s Healthcare Workforce Survey found that administrative overload ranked among the top three reasons clinical and support staff cited for considering resignation. Compensation and flexibility were the other two. Notably, administrative overload was the one factor clinics could address structurally without a budget overhaul.
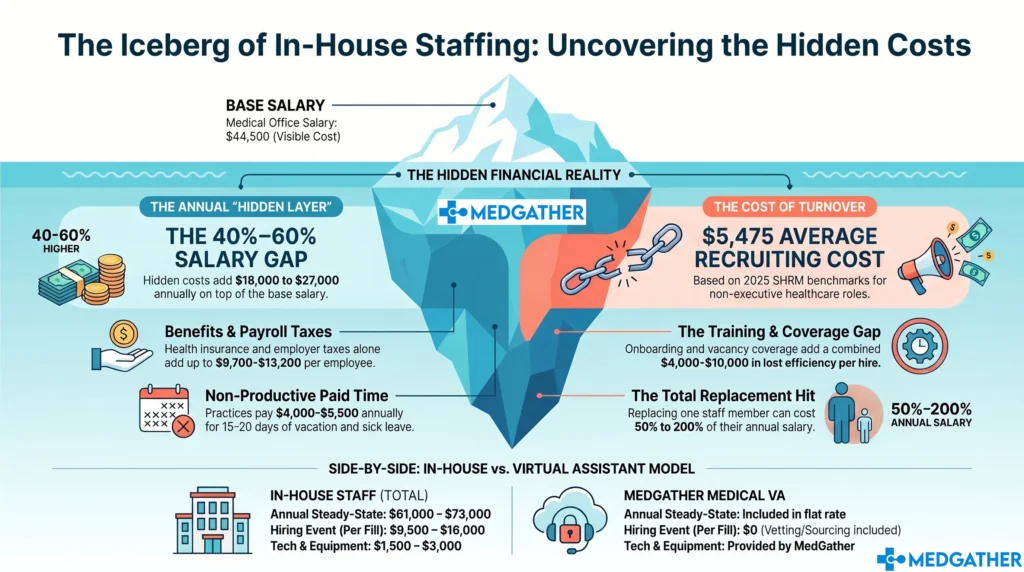
Every resignation carries a real cost that rarely gets calculated directly. Recruiting, onboarding, and productivity loss during the gap add up to anywhere from half to two times a departing employee’s annual salary, according to SHRM research. For a small or mid-sized clinic, that cycle compounds fast, and it tends to repeat because the structural problem that drove the first resignation is still there when the next hire starts.
What Happens When You Stop Relying on the Retraining Cycle
One of the quieter costs in a busy clinic is the retraining cycle. A front desk staff member leaves. The team absorbs the gap while someone new gets hired. The new hire gets up to speed over six to eight weeks, during which errors increase and throughput drops. Two months later, the process starts again because the same workload that wore out the previous person is wearing out this one too.
MedGather’s assistants arrive already trained. They complete MedGather’s onboarding and workflow program before being assigned to any clinic, come in proficient across Epic, Athenahealth, eClinicalWorks, and Modmed, and carry nursing or clinical backgrounds that make them familiar with how healthcare practices actually operate. The adjustment period on your end is minimal because the groundwork is done at the MedGather level before your clinic ever gets involved.
That’s a meaningful difference for a clinic that can’t slow down while someone learns the job. It also means the cost comparison between an MVA and a new in-house hire is not just about hourly rate. It’s about total operational drag, and the MVA model consistently comes out ahead when that calculation is done honestly.
The full breakdown of how the cost comparison actually works covers what most practices undercount when they’re evaluating whether to hire in-house or bring in remote support.
5 Areas Where a Medical Virtual Assistant for Busy Clinics Makes the Biggest Difference
The administrative tasks that create the most friction in a high-volume clinic are predictable. They’re the same ones that show up across practice types and specialties, and they’re the ones that tend to get worse as patient volume grows because the staff-to-task ratio never scales fast enough to keep up.
1. Scheduling and High-Volume Calendar Management
When appointment volume is high, scheduling errors and gaps become expensive in ways that add up quickly. A missed reminder produces a no-show. A cancellation that doesn’t get backfilled is an open slot that could have generated revenue. A booking error that doesn’t get caught until the day of creates front desk scrambling that pulls staff off everything else.
An MVA actively manages the full scheduling cycle: new patient intake, reminder outreach at the intervals that actually reduce no-shows, cancellation handling, waitlist coordination, and calendar hygiene so your team isn’t spending clinic hours fixing booking mistakes. The scheduling tasks a properly scoped MVA can own from day one go deeper than most practices expect when they first start mapping it out.
2. Prior Authorization Follow-Up
High-volume clinics process more authorizations, which means more follow-up, more waiting, and more opportunities for requests to stall in a queue. When prior auth tracking falls to already-stretched staff, it tends to get batched or deprioritized, which means patient care gets delayed by paperwork that could have been cleared days earlier with consistent payer contact.
An MVA owns the follow-up cycle. Requests go out. Status checks happen on schedule. Payer delays get flagged early rather than discovered when a patient calls asking why their procedure hasn’t been approved yet. For a busy clinic processing high authorization volume, that consistency translates directly into faster care delivery and fewer frustrated patients.
3. EHR Documentation and Scribing Support
Documentation is where busy clinics lose the most time they can’t afford to lose. When providers are managing high patient volume, end-of-day charting backlogs become a daily reality. Notes get rushed. Details get missed. And the provider who should have left at six is still at their desk at eight, catching up on documentation that accumulated while they were focused on patients.
MedGather’s assistants come from nursing and clinical backgrounds, which means they understand what they’re documenting. They’re not entering data mechanically. They’re capturing clinical encounters with the context that makes documentation accurate and useful. The specific skills that make this level of scribing support possible start with clinical background and EHR proficiency, not just administrative experience.
4. After-Hours Coverage
Busy clinics don’t stop generating administrative work when the front desk closes. Patient inquiries arrive through the evening. Scheduling requests come in overnight through the website or portal. Prescription questions, referral status requests, and general communications stack up and land on whoever opens the practice the next morning.
That Monday morning backlog is a real operational problem. Staff spend the first hour or two of the week digging out from communications that built up over the weekend, which delays the start of normal workflows before the day has properly begun. MedGather’s after-hours support service keeps that queue from becoming the first problem your team has to solve every single morning.
5. Patient Data Security Without the Compliance Burden
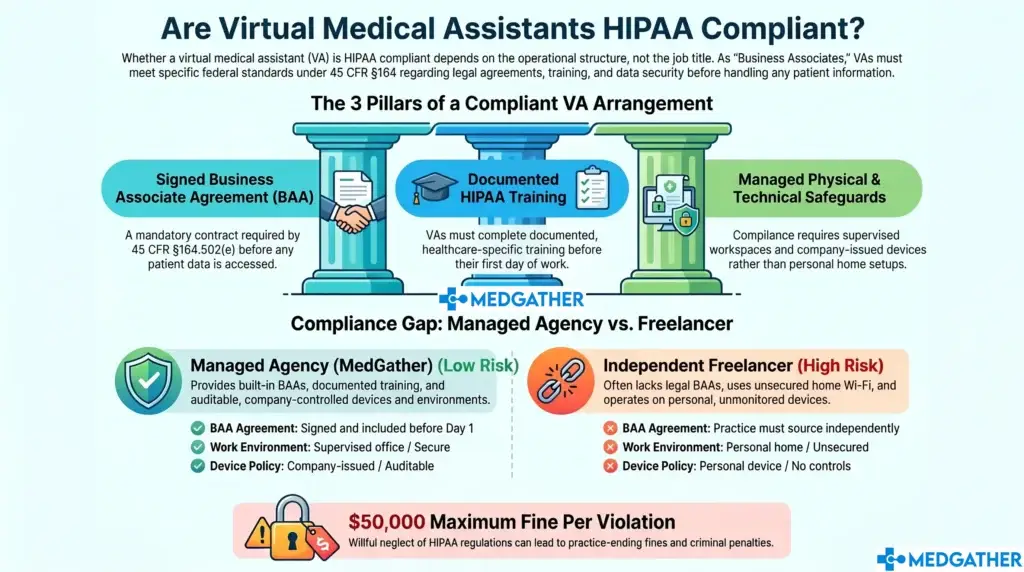
High-volume clinics handle high patient data volume. Every additional access point, every remote worker on a personal device, every unsupervised network connection is a potential exposure. For a busy clinic, adding compliance management on top of operational management is often the thing that pushes an already-stretched team over the edge.
Every MedGather assistant operates from a HIPAA-compliant, supervised workspace with a stable internet connection and a documented backup system. Mandatory compliance training is completed before assignment. A background check is required before any assistant is endorsed to a client. The security structure is built into the model, not delegated to the individual assistant. What separates a compliant virtual assistant setup from one that creates exposure is covered in detail for practices that want to understand the difference before making a decision.
What to Expect When You Bring One In
The practices that benefit most from a medical virtual assistant for busy clinics are the ones where the administrative load has already outgrown the team carrying it. That’s most of the practices that call us.
The transition is not complicated, but it does require a clear starting point. A prioritized task list, provisioned EHR access, and a single point of contact for the first two weeks are what separate a smooth onboarding from one that takes longer than it needs to.
In the first month, the most visible change is usually in scheduling. No-shows drop because reminders are now consistent. The schedule fills more reliably because cancellations get handled the moment they come in. The front desk starts reporting that the pace of the day feels more manageable.
By the 60 to 90-day mark, the structural shift becomes clear. The team is less reactive. Documentation is cleaner. Patient communication is happening without the backlog that used to pile up overnight. The clinic is handling the same or greater patient volume with lower operational stress.
That’s what addressing the structural problem actually looks like. The full picture of what a well-integrated MVA handles and how the model is built is the right starting point for practices that want to understand it before committing to anything.
Built for Clinics That Can't Afford Disruption
Your team gets to focus on patients. Your front desk stops absorbing work that was never theirs to begin with. And your clinic stops losing good staff to a workload that structured support could have absorbed all along.
MedGather was built specifically for practices where the team is stretched thin and the administrative workload has nowhere left to go. Book a free consultation to talk through what relief actually looks like for your clinic.
Is your clinic running on empty?
MedGather's medical virtual assistants come from nursing and clinical backgrounds, are trained before they arrive, and are ready to absorb the administrative layer without disrupting how your team operates.
Frequently Asked Questions
How does a medical virtual assistant help a busy clinic?
A medical virtual assistant for busy clinics absorbs the administrative layer that pulls clinical staff away from patient care. That includes scheduling and calendar management, prior authorization follow-up, EHR documentation and scribing support, after-hours patient communication, and patient data security. By giving each of these workflows a dedicated owner, the clinical team can focus on clinical work and the practice stops losing staff to administrative overload.
Can a medical virtual assistant handle the workload of a high-volume clinic?
Yes, when properly matched and onboarded. MedGather’s assistants come from nursing and clinical backgrounds, arrive already trained on major EHR platforms including Epic, Athenahealth, eClinicalWorks, and Modmed, and complete onboarding before being assigned to any clinic. The adjustment period is minimal because the groundwork is done before your practice is involved. Most high-volume clinics see measurable operational improvements within the first 30 days.