The ROI of Hiring a Medical Virtual Assistant
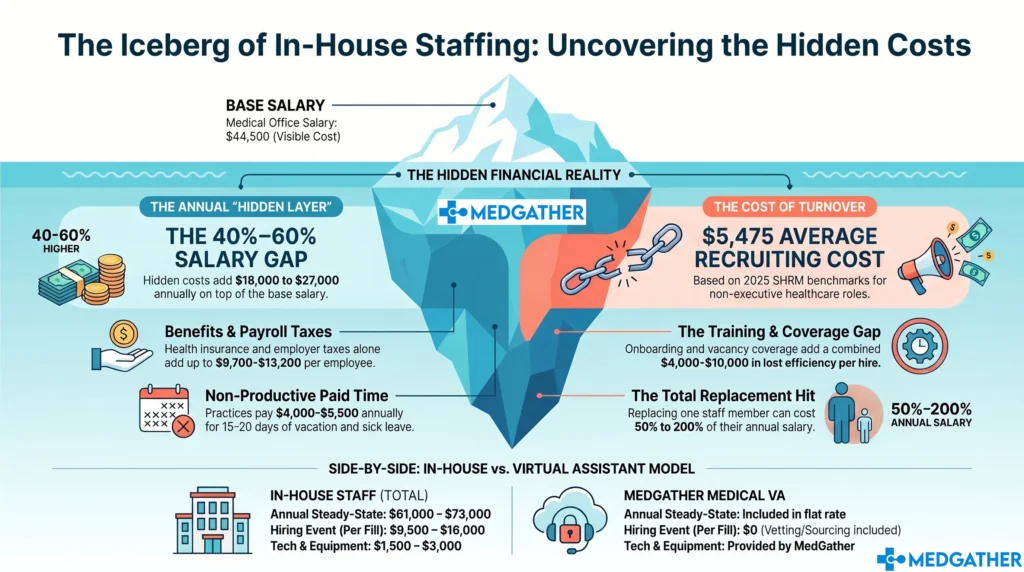
Most conversations about the medical virtual assistant ROI stop at one question: what does a VA cost versus what an in-house hire costs? That comparison answers part of the question, but it misses two larger categories of return that consistently drive the total number higher than practices expect.
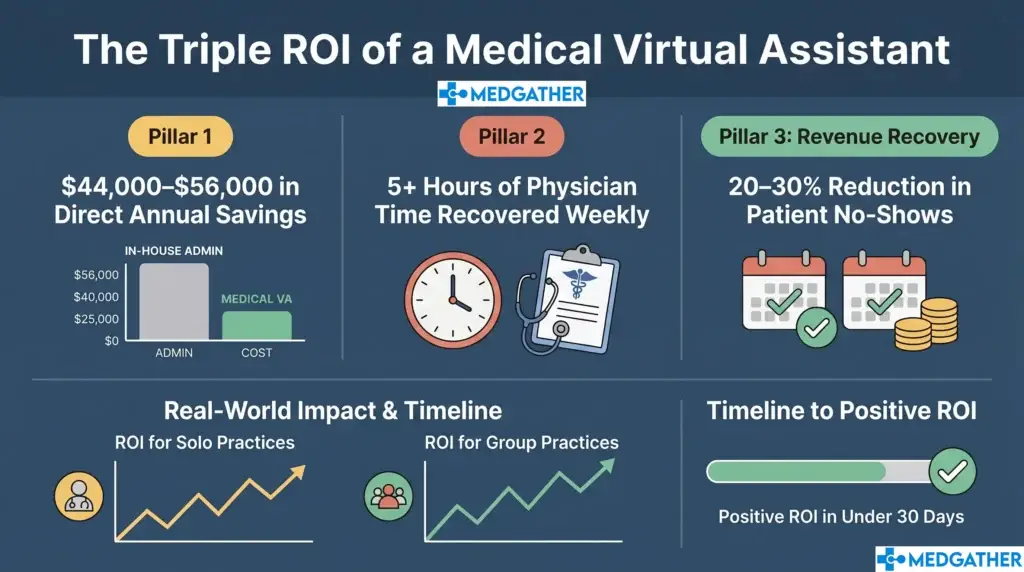
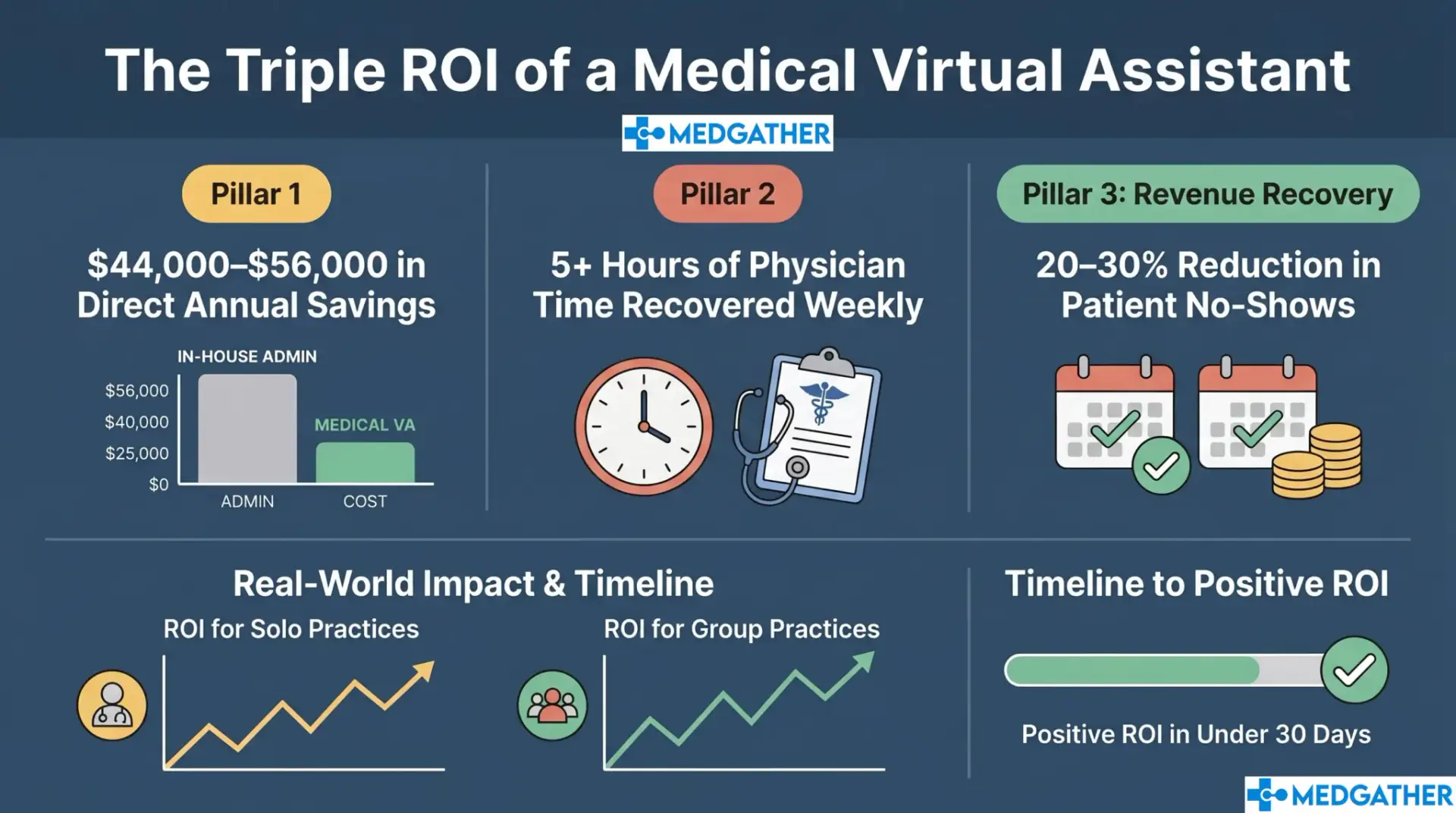
The medical virtual assistant ROI comes from three sources.: direct cost savings, physician time recovered, and revenue that was previously lost through administrative gaps. This guide calculates all three, shows what each looks like with real numbers for two practice sizes, and explains why the cost of a medical VA is rarely the right starting point for the ROI conversation.
TL;DR: What Is the Medical Virtual Assistant ROI?
Solo practice (1 physician, ~80 patients/week): Estimated year-one return of $65,000 to $95,000 from combined cost savings, time recovered, and revenue recovered. Against a VA cost of $18,000 to $30,000 per year, that represents a 200% to 400% return in year one.
Small group practice (2 to 3 physicians, ~200 patients/week): Estimated year-one return of $140,000 to $200,000. Against a VA cost of $24,000 to $40,000 per year, that represents a 300% to 500% return in year one.
These estimates use conservative inputs. Actual ROI depends on patient volume, no-show rates, appointment value, payer mix, and your current administrative structure.
In This Guide
- What does the ROI of a medical VA actually include?
- ROI category 1: Direct cost savings
- ROI category 2: Physician time recovered
- ROI category 3: Revenue recovered through administrative improvement
- The full ROI formula, and how to apply it to your practice
- Two worked examples: solo practice and small group practice
- When does the ROI start showing up?
- How to find out the ROI for your specific practice
What Does the Medical Virtual Assistant ROI Actually Include?
Return on investment in a medical practice context means the measurable financial return relative to what you pay. For a medical VA, the return extends beyond reduced expenses. It includes what you start recovering, from no-shows that get filled, from prior authorizations that go through faster, and from physician time that shifts from administrative tasks back to clinical work.
The three categories this guide calculates:
- Category 1 , Direct cost savings: Reduced staffing cost, elimination of overtime, avoided recruitment and onboarding expense.
- Category 2 , Physician time recovered: Administrative hours returned to clinical work, calculated at the physician’s effective clinical billing rate.
- Category 3 , Revenue recovered: No-show reduction, prior authorization approval improvement, scheduling optimization, and after-hours capture.
ROI Category 1: How Much Does a Medical VA Save in Direct Costs?
The most immediate and easiest-to-quantify return from a medical VA is the reduction in direct administrative staffing costs. According to the Bureau of Labor Statistics, the median annual salary for a medical administrative assistant in the US is approximately $42,000. What that fully loaded cost becomes when employer taxes, benefits, PTO, recruiting, and training are added to, the salary is typically $56,000 to $72,000 per year for a single full-time hire.
Direct Cost Comparison: In-House Admin vs. Medical VA
| Cost Component | In-House Admin (Annual) | Medical VA (Annual) |
| Base salary | $38,000 to $48,000 | Included in monthly rate |
| Employer payroll taxes (7.65%) | $2,900 to $3,700 | None |
| Health insurance contribution | $6,000 to $9,000 | None |
| PTO and sick leave | $1,800 to $3,200 | None , continuous coverage |
| Recruitment cost (per hire) | $3,000 to $8,000 | Included in model |
| Onboarding and training | $1,500 to $4,000 | Pre-trained before assignment |
| Overtime (est. 8 hrs/week) | $8,000 to $16,000 | Eliminated |
| Total annual fully-loaded cost | $62,000 to $92,000 | $18,000 to $36,000 (contact MedGather for custom quote) |
Direct annual savings from switching one full-time in-house admin to a full-time medical VA: estimated $44,000 to $56,000 in year one before time or revenue recovery is included.
| Outbound stat: Bureau of Labor Statistics. Occupational Outlook Handbook , Medical Secretaries and Administrative Assistants. Median annual wage: $47,460 (2024 data). |
ROI Category 2: How Much Physician Time Does a Medical VA Return?
This is the category most practices do not calculate, and it is often the largest single source of return. According to American Medical Association research, physicians spend an average of two hours on administrative tasks for every one hour of direct patient care. In a typical 40-hour clinical week, that represents 13 to 15 hours of weekly administrative time that either displaces patient-facing work or extends the physician’s working day.
When a medical VA absorbs scheduling, inbox management, prior authorization follow-up, and documentation coordination, the efficiency improvement in how clinical time is used typically runs 5 to 10 hours per week per physician. At an effective clinical billing rate of $150 to $300 per hour, that recovered time represents $39,000 to $78,000 in potential clinical revenue per physician per year, even at conservative utilization assumptions.
How Is Physician Time Recovery Calculated?
The calculation uses a conservative estimate of 5 recoverable administrative hours per physician per week, applied at a clinical billing rate of $150 per hour (below the median rate for most specialties) over 50 working weeks:
| Input | Value |
| Admin hours recovered per physician/week | 5 hours (conservative estimate) |
| Working weeks per year | 50 weeks |
| Effective clinical billing rate used | $150/hr (conservative) |
| Annual time value per physician | 5 hrs x 50 wks x $150 = $37,500 |
| At $200/hr (mid-range specialist rate) | 5 hrs x 50 wks x $200 = $50,000 |
| At $300/hr (high-volume or specialist) | 5 hrs x 50 wks x $300 = $75,000 |
Note: This calculation reflects the value of clinical time recovered, not guaranteed additional revenue. It assumes the recovered time is used for clinical work or reduces extended hours. Individual results depend on patient volume and specialty billing rates.
Research Insight: According to the American Medical Association (AMA) , physicians often spend roughly twice as much time on administrative work as they do on direct patient care. Administrative burden remains a significant contributor to physician burnout and operational inefficiency.
ROI Category 3: How Much Revenue Does a Medical VA Recover?
Revenue recovery is the third category, and it compounds the return from the other two. A medical VA generates direct revenue recovery through three mechanisms: no-show reduction, prior authorization approval improvement, and after-hours appointment capture.
No-Show Reduction
The average no-show rate in US primary care practices runs between 15 and 20 percent without systematic reminder outreach. Consistent appointment reminders and confirmation calls reduce that rate by 20 to 30 percent in most practice settings within the first 30 to 60 days. At an average appointment value of $200, even a modest reduction in no-shows produces measurable recovered revenue within the first month.
Prior Authorization Improvement
Denied or stalled prior authorizations represent revenue that is earned at the clinical level but not collected at the administrative level. A VA dedicated to authorization follow-up tracks each outstanding authorization, escalates when payers go quiet, and initiates appeals when denials are received. The improvement in approval rates from dedicated follow-up versus reactive management typically runs 15 to 25 percent, with each approved authorization representing $500 to $2,000 in collected revenue depending on the procedure and payer.
After-Hours Appointment Capture
Patient inquiries and appointment requests that arrive outside clinic hours are often lost in practices without after-hours coverage. An MVA who handles after-hours administrative volume converts inquiries that would otherwise wait until the next morning into booked appointments. For a practice that converts even 10 additional appointments per month at $200 per visit, that is $2,000 per month or $24,000 per year in incremental revenue. How after-hours administrative support works as a service covers what is typically handled during those hours.
Source: MGMA Cost and Revenue Report . MGMA research identifies scheduling failures, prior authorization delays, and other administrative breakdowns as major contributors to revenue cycle leakage in independent medical practices.
ROI Category 3: How Much Revenue Does a Medical VA Recover?
Revenue recovery is the third category, and it compounds the return from the other two. A medical VA generates direct revenue recovery through three mechanisms: no-show reduction, prior authorization approval improvement, and after-hours appointment capture.
No-Show Reduction
The average no-show rate in US primary care practices runs between 15 and 20 percent without systematic reminder outreach. Consistent appointment reminders and confirmation calls reduce that rate by 20 to 30 percent in most practice settings within the first 30 to 60 days. At an average appointment value of $200, even a modest reduction in no-shows produces measurable recovered revenue within the first month.
Prior Authorization Improvement
Denied or stalled prior authorizations represent revenue that is earned at the clinical level but not collected at the administrative level. A VA dedicated to authorization follow-up tracks each outstanding authorization, escalates when payers go quiet, and initiates appeals when denials are received. The improvement in approval rates from dedicated follow-up versus reactive management typically runs 15 to 25 percent, with each approved authorization representing $500 to $2,000 in collected revenue depending on the procedure and payer.
After-Hours Appointment Capture
Patient inquiries and appointment requests that arrive outside clinic hours are often lost in practices without after-hours coverage. An MVA who handles after-hours administrative volume converts inquiries that would otherwise wait until the next morning into booked appointments. For a practice that converts even 10 additional appointments per month at $200 per visit, that is $2,000 per month or $24,000 per year in incremental revenue. How after-hours administrative support works as a service covers what is typically handled during those hours.
Industry Insight: According to the MGMA Cost and Revenue Report , administrative failures in scheduling and prior authorization are among the top contributors to revenue cycle leakage in independent medical practices.
What Is the Full Medical Virtual Assistant ROI Formula?
The ROI calculation combines all three categories into a single framework. Here is the formula used for the worked examples in the next section:
ROI Formula
Total Annual Return = Direct Cost Savings + Time Recovery Value + Revenue Recovered
Net ROI ($) = Total Annual Return − VA Annual Cost
ROI (%) = (Net ROI ÷ VA Annual Cost) × 100
Inputs needed: annual VA cost, patient volume, appointment value, no-show rate, physician count, and clinical billing rate.
What Does the Medical Virtual Assistant ROI Look Like in a Real Practice?
Example 1: Solo Practice (1 Physician, ~80 Patients per Week)
| ROI Component | Estimated Annual Value |
| Direct cost savings (vs. full-time in-house admin) | $38,000 to $52,000 |
| Physician time recovered (5 hrs/wk at $150/hr) | $37,500 |
| No-show recovery (25% reduction at $200/visit, 80 pts/wk x 15%) | $31,200 |
| After-hours and scheduling capture (est. 8 additional appts/mo at $200) | $19,200 |
| Total estimated year-one return | $125,900 to $139,900 |
| VA annual cost (mid-market estimate, contact MedGather for custom quote) | $18,000 to $30,000 |
| Estimated net ROI (year one) | $95,900 to $121,900 | ROI: 320% to 680% |
Example 2: Small Group Practice (2 to 3 Physicians, ~200 Patients per Week)
| ROI Component | Estimated Annual Value |
| Direct cost savings (vs. 1.5 in-house admin FTEs for this volume) | $55,000 to $80,000 |
| Physician time recovered (2 physicians x 5 hrs/wk at $150/hr) | $75,000 |
| No-show recovery (200 pts/wk x 15% no-show x 25% reduction x $200) | $78,000 |
| After-hours capture and scheduling optimization (est. 20 appts/mo at $200) | $48,000 |
| Total estimated year-one return | $256,000 to $281,000 |
| VA annual cost (mid-market estimate, contact MedGather for custom quote) | $24,000 to $40,000 |
| Estimated net ROI (year one) | $216,000 to $257,000 | ROI: 540% to 1,070% |
All estimates are illustrative and use conservative inputs. Actual returns depend on your patient volume, appointment value, specialty, no-show rate, and current administrative structure. These figures do not represent guarantees.
When Does the Medical VA ROI Start Showing Up?
The return from a medical VA does not require a 6-month ramp-up. How quickly a VA integrates into a practice workflow follows a consistent pattern across practice types:
- Days 1 to 30 (no-show reduction and scheduling): The fastest return appears immediately. Reminder outreach and scheduling management produce measurable no-show reduction within the first two to four weeks. Most practices see the impact on the appointment calendar within the first month.
- Days 30 to 60 (inbox, calls, prior auth): Once scheduling is stabilized, the VA takes over inbox management, call overflow, and prior authorization tracking. Staff overtime typically drops during this period.
- Days 60 to 90 (full efficiency, documentation): By the third month, the VA is operating at full capacity across their assigned task scope. Physician time recovery is fully realized by this point. Documentation coordination and referral tracking are running without intervention.
For practices using a managed provider with pre-trained VAs, the ramp-up is shorter than for independently hired VAs, because the assistant arrives knowing the workflows and the platform rather than learning both simultaneously. How MedGather’s model shortens the time to full productivity is consistent across practice types and specialties.
How Do You Find Out the Medical Virtual Assistant ROI for Your Practice?
The ROI calculation in this guide uses market averages and conservative inputs. Your practice’s actual return depends on your specific patient volume, appointment type mix, no-show rate, current administrative structure, and the VA task scope you need. What a structured VA arrangement looks like for your practice type and specialty varies significantly, and the return follows the same variation.
MedGather provides a free strategy consultation that covers your practice’s specific workflows, the VA task scope that makes most sense for your volume and specialty, and a custom quote rather than a generic range. A free consultation is the most direct path to a real ROI number for your specific situation.
Calculate the ROI for your practice
MedGather's free strategy consultation covers your patient volume, task scope, and VA fit , and gives you a real cost and return estimate for your specific practice rather than a market average
Frequently Asked Questions
What is the ROI of hiring a medical virtual assistant?
The medical virtual assistant ROI comes from three sources: direct cost savings (reduced staffing and overtime costs), physician time recovered (administrative hours returned to clinical work), and revenue recovered (no-show reduction, prior authorization improvement, after-hours capture). For a typical solo practice, the estimated year-one return runs $95,000 to $122,000 against a VA cost of $18,000 to $30,000, representing 320 to 680 percent ROI. For a small group practice with 2 to 3 physicians, the estimated return runs $216,000 to $257,000 against a VA cost of $24,000 to $40,000. These estimates use conservative inputs and vary by practice.
How quickly does a medical VA pay for itself?
For most practices, the fastest return comes from no-show reduction, which typically shows up within the first 30 days through systematic reminder outreach. At an average appointment value of $200 and a 25 percent reduction in no-shows for a practice seeing 80 patients per week, that is approximately $31,200 in recovered revenue per year , enough to cover the VA cost in the first few months at the lower end of the market rate range. The full ROI (including time recovery and cost savings) is typically realized by months three to four.
How do I calculate the ROI of a medical virtual assistant for my practice?
Use this formula: Total Annual Return = Direct Cost Savings + Time Recovery Value + Revenue Recovered. Then: Net ROI ($) = Total Annual Return minus Annual VA Cost. ROI (%) = (Net ROI divided by Annual VA Cost) times 100. The inputs you need: your fully loaded in-house admin cost, your patient volume, average appointment value, current no-show rate, number of physicians, and an estimate of the clinical billing rate. If you want a calculation specific to your practice, a free consultation with MedGather will give you a number based on your actual inputs.
Is a medical virtual assistant worth the cost for a solo practice?
Yes, for most solo practices. The math consistently favors the VA model when all three ROI categories are included. Using conservative inputs (5 hours of physician time recovered per week at $150 per hour, a 25 percent no-show reduction on 80 patients per week at $200 per visit, and standard cost savings), a solo practice generates an estimated $95,000 to $122,000 in year-one return against a VA cost of $18,000 to $30,000. The return is proportionally larger for practices with higher appointment values, higher no-show rates before VA engagement, and physicians spending more than 5 recoverable hours per week on administrative tasks.
What is the biggest single source of ROI from a medical virtual assistant?
For most solo and small group practices, physician time recovery is the largest single component when calculated at clinical billing rates. Five hours of physician time per week at $200 per hour over 50 weeks equals $50,000 per physician per year, which often exceeds the total VA cost on its own. However, this category requires the physician to actively redirect the recovered time to clinical work or reduce extended hours. If that reallocation does not happen, no-show revenue recovery (which is direct and does not require physician action) becomes the most reliable first-year return driver.
Sources
- American Medical Association (AMA) . Physician Administrative Burden and Burnout Research. 2023.
- Bureau of Labor Statistics (BLS) . Occupational Outlook Handbook: Medical Secretaries and Administrative Assistants. 2024.
- Medical Group Management Association (MGMA) . MGMA DataDive: Cost and Revenue Report. 2023.