Medical Virtual Assistant Efficiency: 5 Ways Small Practices Get More Done Without Adding Staff
Medical virtual assistant efficiency is not a theory. For solo and small U.S. practices, it shows up in specific, measurable places: a schedule that fills and holds, patient messages that get answered before they become complaints, prior authorizations that do not sit in a queue until they expire, and a provider who finishes the day without three hours of documentation still waiting.
Small practices operate with thin administrative margins. One front desk person covering phones, check-in, scheduling, insurance, and patient follow-up is the norm, not the exception. When that person calls out, gets overwhelmed, or leaves, the whole operation feels it. A medical virtual assistant does not replace that person. It changes the math entirely, adding dedicated administrative capacity without the overhead of another full-time hire.
This post covers five concrete areas where medical virtual assistants measurably improve practice efficiency, with a focus on what that actually looks like inside a solo or small group setting where every hour and every dollar counts.
In This Guide
- Scheduling and no-show reduction
- Patient communication and follow-up
- After-hours administrative coverage
- Staff focus and context-switching
- Compounding efficiency over time
Why Medical Virtual Assistant Efficiency Matters More in Small Practices
A large hospital system absorbs administrative inefficiency across dozens of staff members and departments. A solo practice or small group does not have that buffer. One scheduling gap, one missed prior auth, one afternoon of unanswered patient messages, and the practice feels it in revenue and patient satisfaction at the same time.
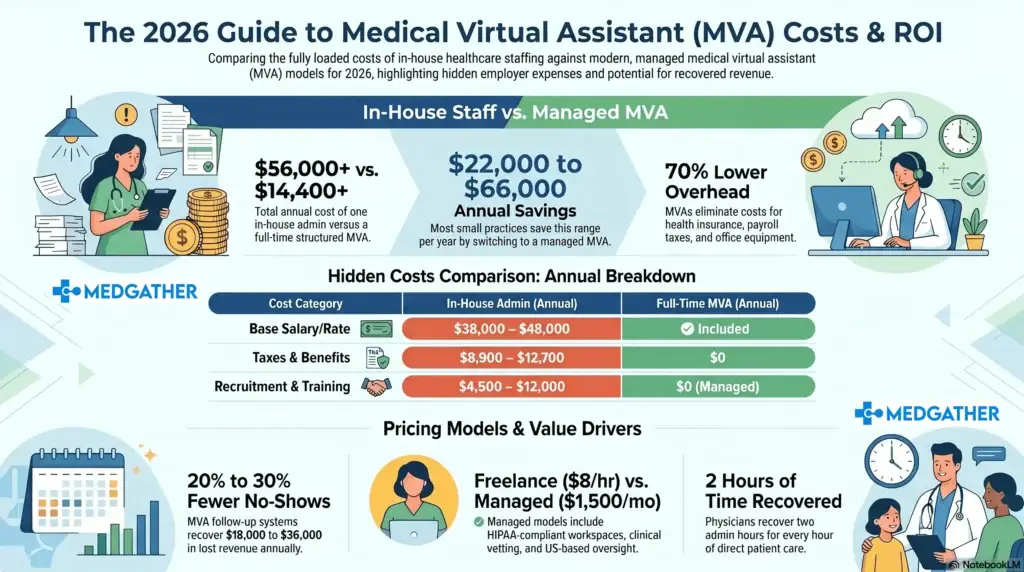
The administrative burden in U.S. healthcare is well-documented. The American Medical Association has reported that physicians spend nearly two hours on paperwork and administrative tasks for every one hour of direct patient care. For a small practice, that ratio means the provider is doing both the clinical and administrative work, usually at the expense of one or the other. The downstream cost of that imbalance goes well beyond provider satisfaction.
A medical virtual assistant targets the specific administrative tasks that drain provider and staff time, handling them with dedicated focus so clinical attention can stay on clinical work. The efficiency gains are not hypothetical. They follow a predictable pattern across the specific workflow categories where small practices consistently lose the most time.
1. Scheduling and No-Show Reduction
Scheduling sounds straightforward until you factor in everything attached to it: new patient intake, insurance verification before the appointment, cancellation handling, waitlist coordination, provider calendar management, and the reminder outreach that determines whether patients actually show up.
In a small practice, all of that typically lands on whoever picks up the phone. The result is a scheduling function that is reactive rather than systematic. Appointments get booked but reminders get skipped. Cancellations open slots that do not get refilled because no one has time to work the waitlist. No-shows accumulate, and the schedule ends the week with gaps that directly affect revenue.
A dedicated MVA takes ownership of the full scheduling cycle. Reminders go out consistently, by phone or message, at the intervals that research shows actually reduce no-shows. Cancellations trigger immediate outreach to the waitlist. New patient intake gets completed before the visit rather than at the front desk on arrival, which shortens check-in and improves the patient experience from the first contact.
MGMA data consistently shows that proactive appointment reminders reduce no-show rates by 20 to 30 percent in primary care settings
Practices that have worked through what a medical virtual assistant can actually take off the scheduling plate typically find the list longer than expected. Scheduling is one entry point. The full scope of what transfers is considerably wider.
2. Patient Communication and Follow-Up
Patient communication is where small practices most visibly fall behind when administrative capacity is stretched. Messages go unanswered for longer than they should. Follow-up calls after appointments do not happen consistently. Prescription refill requests sit in a queue because no one has a dedicated window to process them. The clinical team knows the follow-up should happen. There is just no one whose primary job it is to make sure it does.
An MVA handles the communication layer that falls between clinical care and front-desk operations. That means portal message triage and routing, outbound follow-up calls after visits, prescription refill coordination, referral status updates to patients, and general inquiry responses that do not require clinical judgment but do require prompt, professional handling.
The efficiency gain here is twofold. First, patients get faster responses, which reduces callbacks, complaints, and the kind of patient dissatisfaction that eventually shows up in reviews. Second, the clinical team stops absorbing administrative communication that pulls them away from patient care. Those interruptions add up fast in a small practice where the provider is already the bottleneck.
For practices that see high patient message volume outside regular hours, extending that communication coverage into evenings and weekends removes a significant source of unanswered requests that compound by Monday morning.
3. After-Hours Coverage: The Efficiency Gap Most Small Practices Ignore
For a solo or small group practice, the administrative day does not end when the office closes. Patient messages arrive through the evening. Appointment requests come in after hours through the website or patient portal. Prescription questions, referral inquiries, and general communications stack up overnight and land on whoever opens the practice the next morning.
The Monday morning backlog is a real operational problem. Staff spend the first one to two hours of the week clearing communications that accumulated over the weekend, which delays the start of normal workflows, pushes scheduling tasks back, and creates a reactive opening to a week that needs to be proactive to run well.
An MVA with after-hours coverage handles that communication as it arrives. Urgent messages get triaged and routed appropriately. Appointment requests get captured and scheduled. Non-urgent inquiries get acknowledged so patients are not waiting for a response until the following business day. The practice opens on Monday to a cleared queue rather than a backlog. That difference, particularly in how it affects practice workflow from first thing in the morning, is something most small practices only appreciate after experiencing it for a few weeks.
The efficiency case for after-hours coverage is not just about the messages themselves. It is about the operational rhythm of the practice. A small practice that starts every day already behind never quite catches up. One that starts with a clean slate has a fundamentally different week.
4. Staff Focus and the Hidden Cost of Context-Switching
Context-switching is one of the most underestimated sources of administrative inefficiency in small practices. When one person handles phones, scheduling, insurance verification, patient check-in, and follow-up simultaneously, they are not doing any of those tasks at full capacity. Each interruption requires a mental reset. The accumulated cost of those resets across a full day is significant, even if no individual interruption looks particularly disruptive.
Research on task-switching consistently shows that it takes an average of 23 minutes to fully return to a task after an interruption. In a small practice where the front desk person is interrupted every few minutes by incoming calls, walk-ins, and provider requests, the math works out to a staff member who is rarely, if ever, operating at full productive capacity on any single task.
An MVA reduces the number of tasks competing for the same person’s attention. When scheduling, prior authorizations, and patient follow-up have a dedicated owner, the in-office staff can give full attention to what is in front of them. Check-in gets smoother. Provider support becomes more consistent. The practice runs at a higher baseline efficiency without adding headcount or asking anyone to work faster.
This is one of the reasons small practices that move to a virtual assistant model consistently report improvements in staff retention alongside the efficiency gains. When staff are not perpetually overwhelmed, they stay longer. And staff turnover is one of the most expensive operational costs a small practice carries.
5. How Medical Virtual Assistant Efficiency Compounds Over Time
The efficiency gains from an MVA are not static. They build on each other in ways that take a few months to fully appreciate but become very clear once the practice has experienced them.
In the first few weeks, the most visible improvement is usually scheduling. No-shows drop because reminders are now consistent. The schedule fills more reliably because cancellations get handled immediately. That improvement in schedule density has a direct revenue effect that shows up quickly.
Over the following months, the compounding happens at the workflow level. Staff are less reactive because the communication backlog is no longer a daily problem. The provider gets cleaner handoffs because documentation support has removed the end-of-day charting burden. Patient satisfaction improves because follow-up is now systematic rather than sporadic.
By the six-month mark, practices typically report that they are handling more patient volume at the same staff headcount, with lower operational stress across the team. That is the compounding effect of building remote administrative capacity into the practice structure rather than adding it as a reaction to overload.
What that looks like practically will vary by practice type and specialty. Understanding where a medical virtual assistant fits into your specific workflow is the right starting point before committing to a scope or structure.
What to Realistically Expect in the First 90 Days
Efficiency gains from an MVA do not happen overnight. The first two weeks are almost always spent on onboarding: system access, workflow documentation, communication protocols, and learning the specific preferences of the practice and providers. This period requires some investment of time from the practice side, and practices that skip it tend to get slower results.
From weeks three through six, the MVA moves into independent execution. Scheduling, patient communication, and after-hours coverage stabilize. The practice starts seeing the operational effects, though measuring them takes a few more weeks of baseline data.
By the 60 to 90 day mark, most small practices have a clear picture of what has improved and what still needs adjustment. This is the point where the MVA arrangement either gets expanded because the value is evident, or refined because specific workflows need a different approach.
A structured onboarding process and clear workflow documentation from the start is what separates a smooth 90-day ramp from one that drags on without producing measurable results. The efficiency gains are real. The timeline to reach them depends almost entirely on how well the engagement is structured at the beginning.
The Efficiency Case Is Practical, Not Theoretical
Small practices do not have the administrative slack that larger systems absorb. Every hour lost to inefficiency is an hour that could have gone to a patient, a provider, or a workflow that needed attention. Medical virtual assistants close that gap in specific, predictable ways: a schedule that holds, patient communication that happens consistently, after-hours coverage that prevents Monday backlogs, and staff who can focus instead of context-switch through the day.
The right starting point is understanding which of those areas costs your practice the most right now. The full picture of how the medical virtual assistant model works gives context for making that assessment. And if you already have a clear picture of the problem and want to talk through whether MedGather is the right fit, the conversation is a straightforward one.
By the 60 to 90 day mark, most small practices have a clear picture of what has improved and what still needs adjustment. This is the point where the MVA arrangement either gets expanded because the value is evident, or refined because specific workflows need a different approach.
A structured onboarding process and clear workflow documentation from the start is what separates a smooth 90-day ramp from one that drags on without producing measurable results. The efficiency gains are real. The timeline to reach them depends almost entirely on how well the engagement is structured at the beginning.
Ready to see how MedGather fits your practice?
Book a free strategy call — no obligation. A real conversation about what your practice needs.
Frequently Asked Questions
How do medical virtual assistants improve practice efficiency?
Medical virtual assistants improve practice efficiency by taking ownership of specific administrative workflows that consistently consume provider and staff time: scheduling and reminder outreach, patient communication and follow-up, after-hours message triage, and prior authorization coordination. In small practices, these tasks are often spread across the same one or two people who handle everything else. A dedicated MVA gives each workflow a focused owner, which reduces errors, speeds turnaround, and frees clinical staff to focus on patient-facing work.
How long does it take for a medical virtual assistant to improve efficiency?
Most small practices see meaningful efficiency improvements within 30 to 60 days of a properly structured MVA engagement. The first two weeks typically focus on onboarding and workflow setup. By weeks three through six, scheduling, patient communication, and after-hours coverage are running consistently. The compounding efficiency gains, where improvements in one area reduce friction in others, generally become clear by the 90-day mark.